What to Expect
- Home
- What to Expect
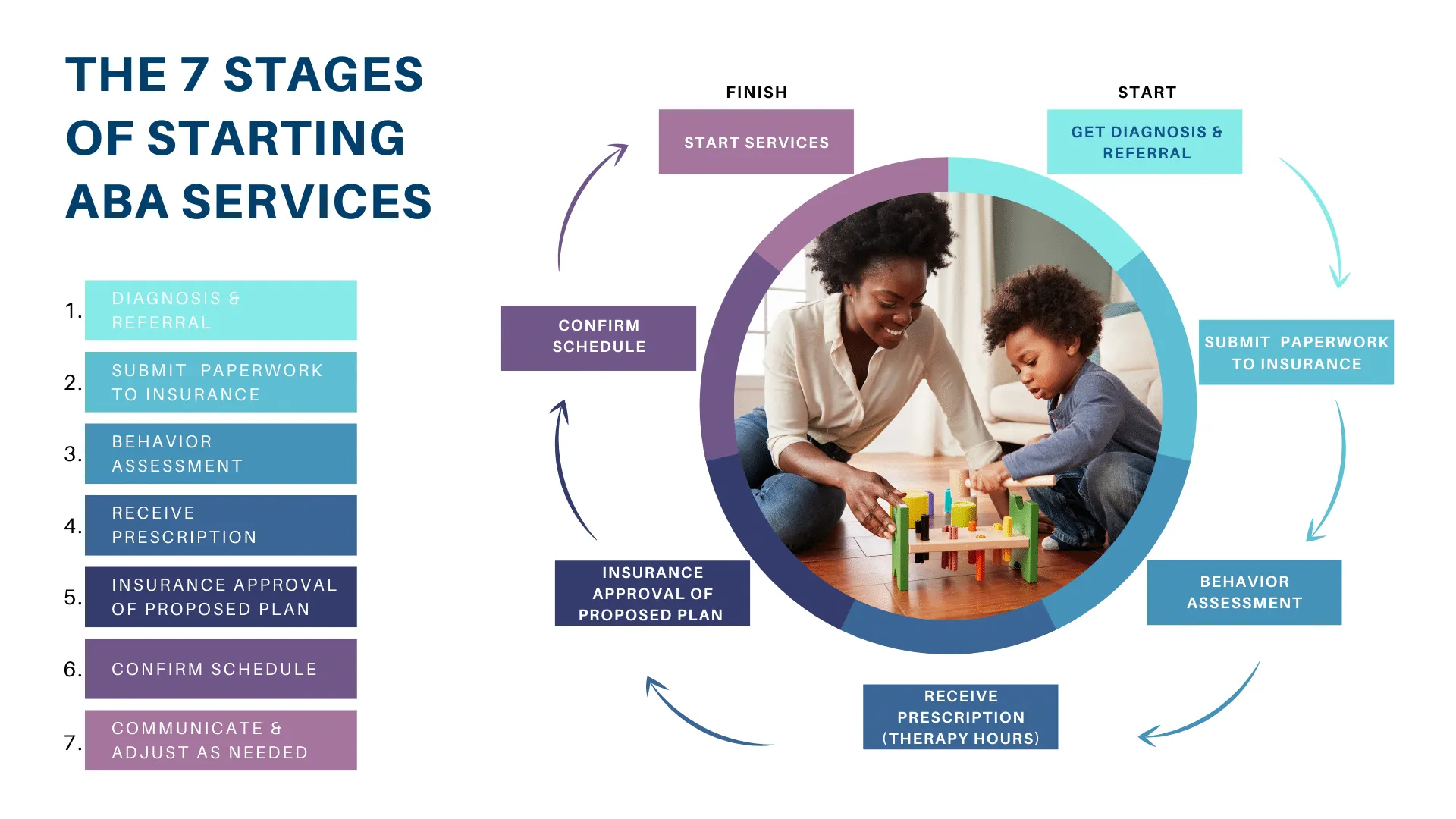
As of now, the only BCBA (Board Certified Behavior Analyst, also referred to as a BA) for BTR (Beyond the Rainbow) is me, Casey, but additional BCBAs may be hired in the future. Once I’ve spoken to you and you decide you do want to have Beyond the Rainbow provide ABA for your loved one, I will schedule to meet with you 1-2 times, going over intake paperwork, explaining ABA and answering questions, and reviewing company policies and providing a more in-depth look at “how it works,” giving you a handbook to refer to. Since it is a lot of information to absorb, a couple different appointments may be best so it’s not information overload! Then, I will schedule the assessment, which will involve a caregiver interview and direct assessment. Unless a client is taken on in a location far outside my core base in Chester County (such as a possible remote case in NC), all assessments and reassessments will be conducted in person, not virtually. After the assessment, I will create goals for your loved one and write up a report (this may take 1-2 weeks). I will share this report with you for your approval (and the feedback of the client, when possible) before submitting it to the relevant insurance company.
Then, as we wait for approval from your insurance, I will look for a therapist who is a good fit for your child. (Some of this may vary if services are for a teen or adult.) In most cases with hiring, people who are looking need a job as soon as possible and are not able to wait for a job that is weeks or so out. Also, I value finding a therapist that will be a good fit for your family and child. (Different people have different strengths.) Due to this, BTR will generally need to secure a client first and know what personality will be a good fit for them instead of hiring someone first who must wait on a client and then just plug them in with whatever kiddo gets approval first. Some kids do better with a person that has a calm energy and quiet voice whereas others need a therapist with high energy who can be goofy. Some therapists will have more experience or be more comfortable with little kids whereas others will be more suited to older kids. Some therapists may not be comfortable with diapers or clients with physical aggression, regardless of provided training. All of these variables will be a part of the hiring process to help prevent wasting precious time trying to build rapport with a therapist that isn’t going to be a good fit and then having to pause services to find someone else, only to start the pairing process all over again.


You will have one or two therapists, referred to as BTs (Behavior Technicians), depending on how many weekly hours your child is scheduled for. Therapists must be at least 18, have a high school diploma or GED, and pass a criminal background check and abuse registry. They will be trained to become RBTs (Registered Behavior Technicians), which requires 40 hours of training and passing a competency exam from the BCBA (me) before them passing an exam offered by the BACB (Behavior Analyst Certification Board). Your BT(s) will come to your home to deliver in-person direct care. As your BCBA, I’m allotted a certain percent of hours to supervise and train (generally 10-20%) based on the amount of direct care provided. For example, if your child receives 15 hours of direct care weekly and I can bill 10% of what the direct care hours are, I will generally have 1.5 hours weekly to supervise as a BCBA. If a therapist or the family cancels sessions and is unable to make them up, that will decrease the amount of hours I have to supervise. I will always be present at the first session, but I may conduct some supervision remotely. This can be useful for clients who are more distracted with more people or have higher anxiety levels when there are too many people. It can also be a helpful way to supervise and train so that the therapist takes initiative and doesn’t become prompt dependent on me taking over, allowing me to see how they are doing things when I’m not there to physically assist.
Perhaps you’ve had ABA before and wonder more about my approach as a clinician. At the heart of it, I try to be FUN. Life is hard enough, and I don’t want to send people through your doors who, in the big scheme of things, make life harder. I prioritize the rapport-building process. Establishing trust, not just between the therapy team and your loved one, but also with you, the caregivers, is essential. I’m knowledgeable on the research behind recommended weekly ABA hours (generally 25-40 for young children), but I’m not blind to the logistics. For example, if your kid is in school all day, we will figure out a plan that allows progress while not sending your kiddo straight into burn out and making ABA an aversive experience to dread daily. That would defeat the entire point! I prioritize NET (natural environment training that embeds learning opportunities in a child’s everyday routines and environment). For example, instead of sitting at a table and going through flash cards to teach body parts, we may play with dolls on the floor and suddenly Ariel gets hurt when she loses her tail to become a human and stumbles walking on the imaginary sand. The therapist may point to Ariel’s foot while saying, “Oh no! Ariel tripped on a rock and hurt herself! What body part is this?…..Yes, her foot! Call a doctor and tell them to bring bandages for her foot!” Although there is a time and place for skills taught at a table, you will not see your child drilled at a table for the majority of a session—ever! I’m not into “copy and paste” cookie-cutter programming. I strive to use the personal interests of my clients to fashion individualized goals in creative ways, asking them questions as well to gain their feedback whenever possible. If they are not yet equipped to communicate with me in a clear way, I’ll watch their nonverbal behavior, which will convey a lot!

No matter how much experience a clinician has, none of us are wizards (unfortunately, because who wouldn’t love a little magic?). There is always an element of trial and error and exposing kids to new experiences. The trick is to find the balance of giving something enough time to see if it works but not too much time and the humility to notice and admit when it’s NOT working! And when it comes to expanding a kid’s repertoire of things they enjoy (activities or toys), one must find the balance of ensuring a kid has been taught HOW to play with a certain toy or how to engage in a certain activity, and then know when to accept that a kid is just not into it and move on. Interests evolve so what doesn’t work or isn’t an interest today may change in the future, but being flexible and not rigid (much as we teach the client) is pivotal in order to be a good clinician.
Will every moment be fun? No, and if they were, sessions would clearly be devoid of building certain skills NECESSARY for thriving in the real world. Some days will be better than other days, such is life, and there will be challenges and frustrations, but the challenge will also meet your loved one where they are so they can simultaneously be taught emotional regulation to help equip them with successfully facing inevitable challenges throughout their lives. These skills and conflict-resolution skills will also be a part of the required parent training (insurance typically requires 2 parent goals that demonstrate caregivers are participating in therapy and learning as well). We as adults cannot instill skills into our children that we do not have ourselves or model consistently. There will also be times that will be hard for the caregivers as they work on establishing healthier behavioral responses to their loved one’s challenging behaviors. For example, if a parent has established a pattern of telling a child “no” to a request, but when that child tantrums, the parent gives in, that has taught the kid that crying/screaming/throwing things works at getting them what they want so they’ll continue using that tactic.


If that parent now rocks that kid’s world by no longer allowing those behaviors to work and follows through with their “no,” the family can expect those behaviors to escalate at first. Why? If the kid is used to screaming being effective and suddenly it no longer is, that’s a shock, so not only is it upsetting, but maybe they think that adding on some extra discomfort for the parent will now be necessary to achieve their goal (overriding that “no”), such as hitting their parent. Seeing your child upset, regardless of the reason, is always unpleasant for a parent, but avoiding real life scenarios during sessions that trigger challenging behaviors would result in the loss of opportunities for the client to implement the emotional regulation strategies they are being taught. Allowing challenges to occur naturally during sessions also allows therapists to model strategies for caregivers and coach them and the child through the event. A lot of challenging behaviors also occur because a child does not have a way to functionally communicate their preferences, needs, or feelings. Sign language (if fine motor skills are strong) and the use of pictures (PECS is often used, which stands for Picture Exchange Communication System, and AAC devices, which stands for Augmentative and Alternative Communication) have been shown to promote the development of vocal language, and once consistent progress is made, such tools can be faded out.
There are companies that don’t put their focus on parent training, especially when services are conducted solely in clinics and parent training is typically limited to one hour per month. I will be up front in stating that I believe parent training to be one of the most critical components to ABA intervention making the largest strides of progress and that progress not dragged out slowly. There are certainly many variables that affect progress, including assessing comorbidities and cognitive impairments, but the caregivers are the ones with the child most often and the most influential people in a child’s life. If caregivers are not performing the same strategies the ABA team is with consistency, they will not only hinder progress, but can also downright unravel it. Having in-home services allows therapists to model procedures and coach caregivers from the sidelines on a regular basis.


Afterall, the goal is not to have tons of therapists inside your home forever, but to make significant gains and equip the family in such a way that we are not needed there anymore! This does not require a caregiver to follow the therapist around every second of a session, but it does require some daily participation, which will also ensure that goals generalize. If your kid can demonstrate desirable skills and emotional control with the therapy team but not with their family once we leave, what good is that? BTR is willing to work with different family dynamics (e.g., maybe one parent works most of the time, but could they be present for a weekend session twice a month?). For a family that is struggling but wants to be a part of the process, even if they don’t yet know how, BTR can help; however, if being an active member in the therapy process is not something you desire or are even willing to do, we may not be the best provider for you.
I will be there to answer questions, explain the “why” behind any recommendations I give, and support families and direct care therapists through the process. Having worked many places over the years and having 3 former bosses who have been arrested for unethical practices, I’m keenly aware of the common problems that exist in this field and will openly discuss any concerns you have. Some of these common problems will be things I will not tolerate (such as sending therapists in whom have not received training or not providing adequate supervision and ongoing training), and others are problems felt by pretty much everyone in this field that I will do my best to prevent while maintaining transparency (such as turnover rate with direct care therapists). As a human with limitations, I acknowledge there may be inconveniences with services at times, such as a therapist cancelling when sick or having car trouble, but I do promise to always be real with you, address concerns head on, and keep you updated while providing honest information and answers to questions. I dedicate myself to listening to families, understanding their needs, and delivering real solutions that improve quality of life—not just for the children, but for the entire household.
